Ultrasound Resources for Family Physicians
Bedside ultrasound or POCUS (point-of-care ultrasound) is essential to the full-spectrum family medicine physician. Only now is formal training becoming universally done in medical schools and Family Medicine residencies. It’s never too late to learn! My dream is that every family physician is an expert in POCUS. Here are some resources I’ve found helpful in learning ultrasound.
Ultrasound Guides:
Presentations I’ve done nationally and guides for beginners:
- Ultrasound for the Uninitiated: Hacks to Learn Ultrasound Quickly & Efficiently
- POCUS with Purpose: High-Impact Scans Every Family Doc Should Know
- Top Free Ultrasound Learning Resources
- Abdominal Aortic Screening Protocol
- POCUS DVT Protocol
- Lung Scanning Protocol
- Lung US Literature Review
Family Medicine Ultrasound Pathology Library:
These slides are primarily notes for myself as I learn and deepen my understanding of ultrasound but many folks have found these cases helpful so I present them here. I collect interesting cases and pathological scans and compare them to normal. I label images and overlay lines and shapes to help learners identify structures. I also include relevant literature.
Example case 1:
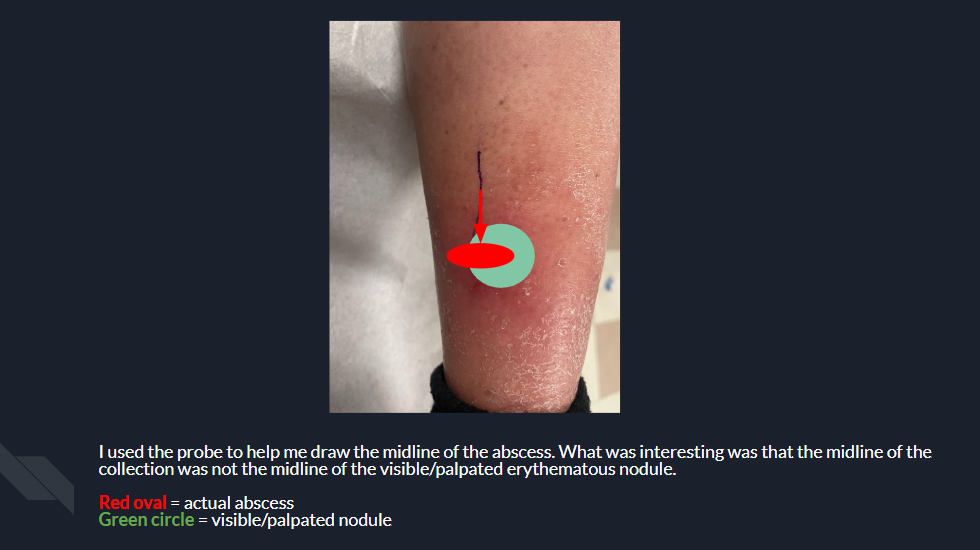
66 yo F w/ a PMH of T2DM, OA, HTN, tobacco use p/w 1 week of red, swollen right calf. Has chronic edema but this is worse than normal. No pus or drainage. No injury to the leg or fall recently. No h/o surgery of her legs except for a h/o right knee replacement. No fevers. No recent travel or prolonged immobilization. No h/o leg infection before

Example case 2:
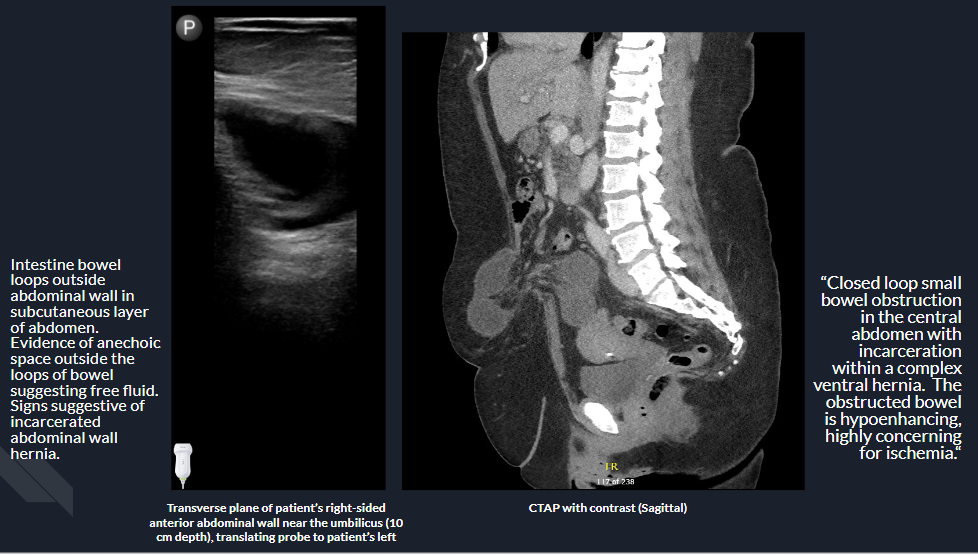
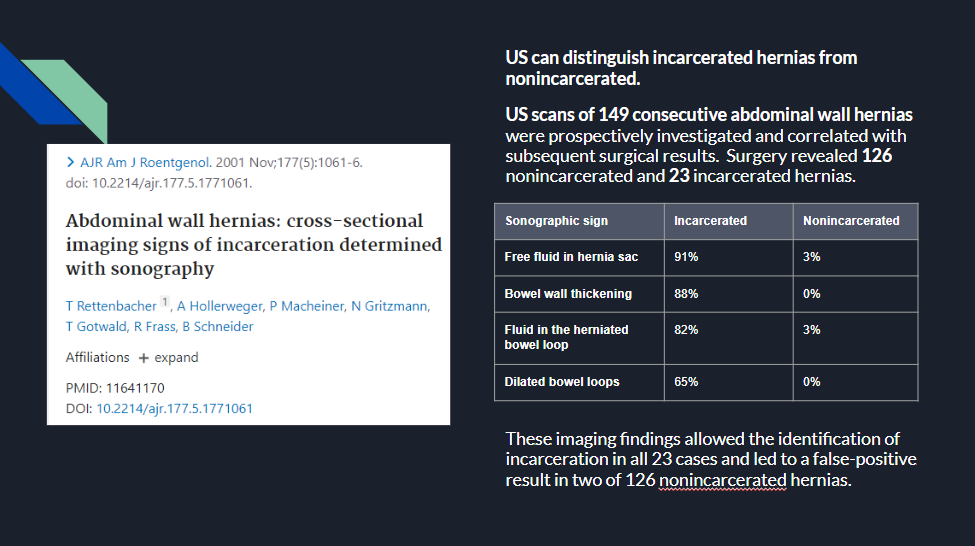
40 yo F w/ a h/o c/s p/w to the clinic for abdominal pain and vomiting bile. 10-15 cm soft mass protruding from anterior right side of abdomen on exam that was very tender. Bedside US done showing:
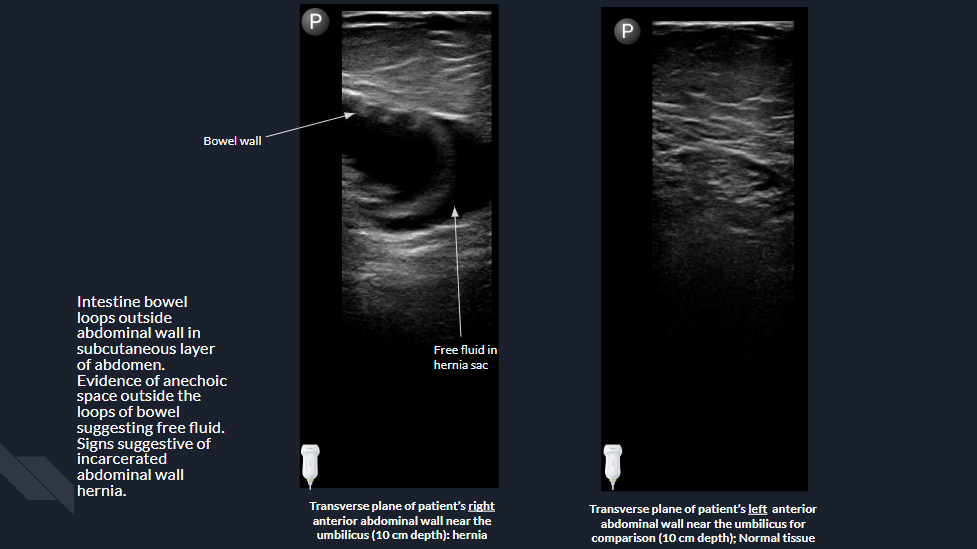
Signs of incarceration on US with possible strangulation so sent to the ED from clinic. Lactate 2.4, WBC 13. CTAP showing evidence of incarcerated ventral hernia with question of intestinal hypoperfusion. Bedside reduction attempted by surgery but not successful. CT angiogram done showing persistent hernia and “Essentially unchanged appearance of thickened hypoenhancing obstructed mid small bowel loops with two discrete transition points consistent with a closed loop obstruction and partial herniation into a complex ventral hernia.” Went to surgery for exploratory laparotomy, lap assisted small bowel resection and incisional hernia repair. 70 cm small intestine resected.
Example case 3:
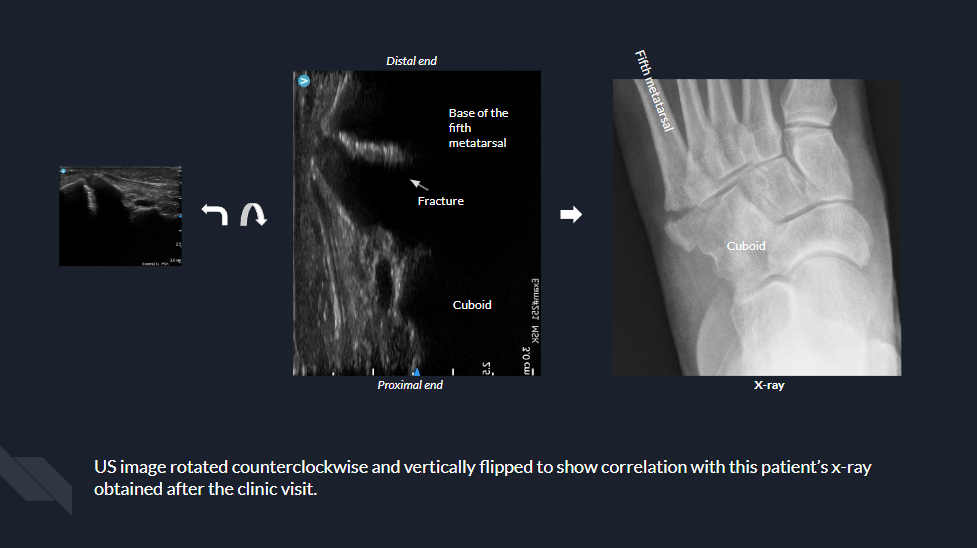
61 yo F p/w after inversion injury. Swelling and bruising of lateral foot. Tender to the base of the fifth metatarsal. Bedside US done.

Fracture on US. XR to confirm. Possibly articular on read. Boot, ortho referral.